

A hospital mattress is not simply an accessory placed on top of a hospital bed. It is the support surface that remains in continuous contact with the patient and influences pressure distribution, comfort, temperature, moisture, movement and positioning.
The right mattress cannot prevent every pressure injury or replace clinical care. It can support a wider prevention strategy when it matches the patient’s risk, mobility, body dimensions and care environment. The wrong mattress can create safety and workflow problems even when the hospital bed itself is well designed.
Hospitals comparing medical mattresses and support surfaces should therefore evaluate the bed, mattress, patient and care protocol as one connected system.
In This Guide
How to choose a hospital mattress
What a hospital support surface does
How foam, viscoelastic and air systems differ
Why repositioning remains necessary
How mattress and bed compatibility affects safety
How Optium mattress models compare
What procurement teams should check
Common purchasing mistakes
Frequently asked questions
Quick Answer: Which Hospital Mattress Should a Facility Choose?
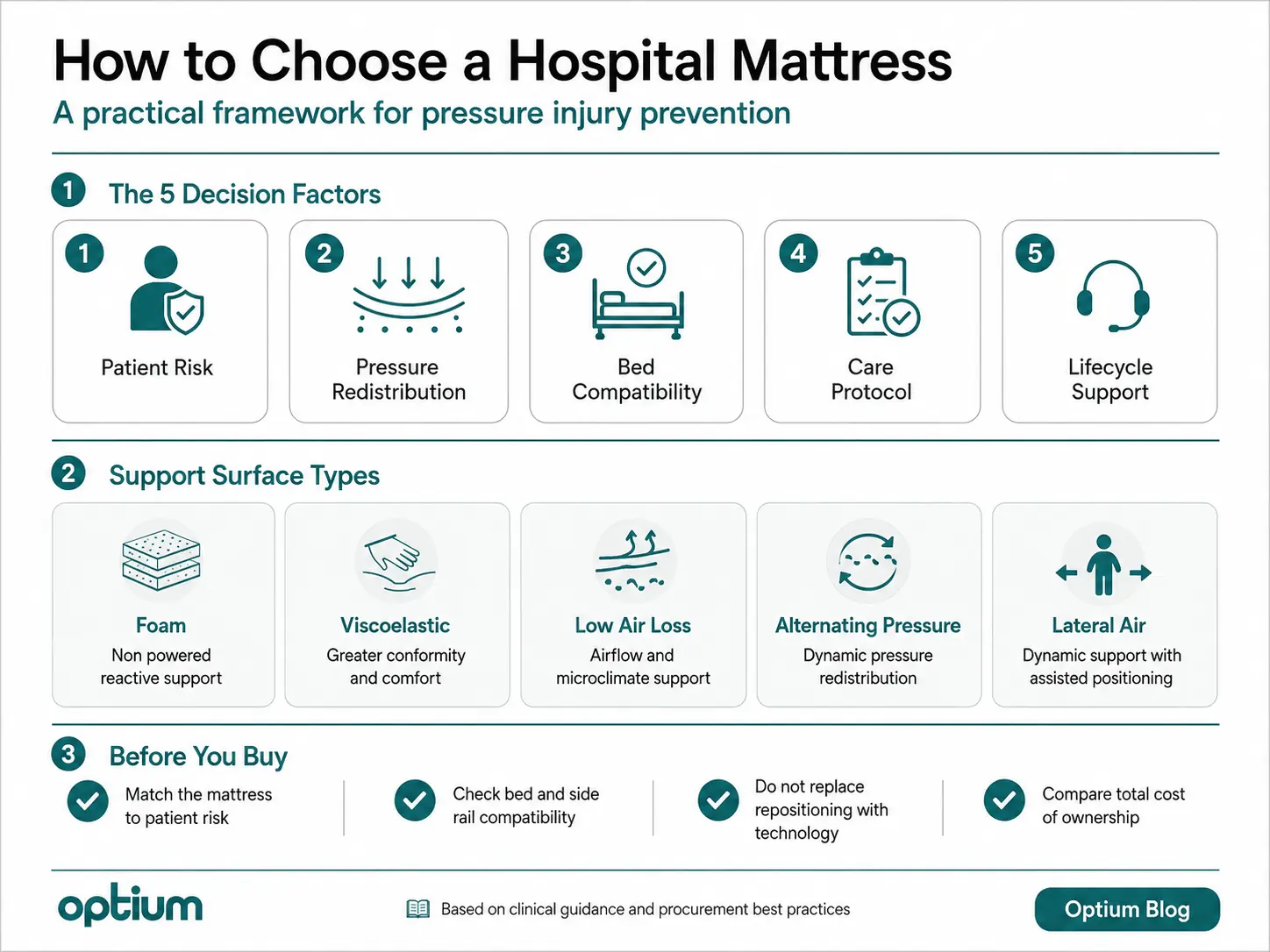
Hospitals should select a mattress through five decisions:
Assess the patient: Consider mobility, sensation, existing skin damage, moisture, nutrition, body dimensions and the ability to reposition independently.
Define the clinical objective: Decide whether the surface is required primarily for general support, pressure redistribution, microclimate management, alternating pressure or assisted lateral positioning.
Confirm bed compatibility: Check length, width, thickness, fixation, side rail geometry and the ability to follow bed movements.
Review the care protocol: The mattress must work with repositioning, skin inspection, continence management, nutrition, mobilisation and patient transfer procedures.
Evaluate lifecycle support: Compare covers, pumps, alarms, replacement cells, training, cleaning requirements, spare parts and expected downtime.
A more advanced mattress is not automatically a better mattress. The correct choice is the surface that fits the patient group, hospital bed and way care is delivered.
What Is a Hospital Support Surface?
A hospital support surface is a specialised mattress, overlay or integrated system designed to redistribute pressure and help manage friction, shear and the microclimate between the patient and the surface.
The current full body support surfaces chapter of the NPIAP, EPUAP and PPPIA International Pressure Injury Guideline was produced jointly by the National Pressure Injury Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance.
The fourth edition chapter, edited by Emily Haesler and updated in May 2026, describes support surfaces as systems designed to redistribute pressure, reduce friction and shear, and assist with microclimate management.
These functions are related, but they are not identical.
Pressure redistribution concerns how mechanical load is spread across the patient’s body.
Envelopment describes how closely the surface conforms to the patient’s shape.
Immersion describes how deeply the patient sinks into the support surface.
Microclimate management concerns temperature and moisture at the interface between the patient and the mattress.
A mattress should therefore be selected according to measurable characteristics and patient requirements, not only according to a familiar product category name.
What Does the Current Clinical Evidence Say?
The NPIAP, EPUAP and PPPIA guideline strongly recommends a pressure redistribution foam support surface for individuals at risk of pressure injuries, although the certainty of the evidence is classified as low.
Its evidence analysis estimated 106 fewer pressure injuries per 1,000 individuals when pressure redistribution foam was compared with foam without pressure redistribution properties.
The guideline also provides an uncertainty range of 135 fewer to 58 fewer injuries per 1,000 people. This matters because the statistic should not be presented as a guaranteed result for every hospital or patient group.
The practical conclusion is not that every patient requires the same foam mattress. It is that foam without appropriate pressure redistribution properties should not be treated as an adequate default for an at risk patient.
How to Choose a Hospital Mattress for Pressure Injury Prevention
Begin With Patient Risk, Not Product Technology
The starting point should be a structured clinical assessment.
Important factors include:
The patient’s ability to move and change position
Existing pressure injuries or previous skin damage
Reduced sensation or impaired circulation
Exposure to moisture and perspiration
Nutrition and hydration status
Body weight and body dimensions
Expected length of stay
The ability of caregivers to reposition the patient safely
NICE guidance on pressure ulcer prevention recommends pressure redistribution equipment for people at high risk. It also recommends a high specification foam mattress for adults admitted to secondary care and adults assessed as being at high risk in other care settings.
A mattress category should never replace clinical judgement. Two patients in the same ward may require different support surfaces because their mobility, skin condition, comfort and care requirements are different.
Define the Clinical Objective
Procurement teams should establish what the mattress is expected to achieve.
A reactive foam surface may be appropriate when the priority is continuous pressure redistribution without a pump.
A viscoelastic surface may be evaluated when greater envelopment and comfort are required.
An air system may be considered when the clinical objective includes pressure redistribution, microclimate management or programmable pressure changes.
An alternating pressure system changes which areas of the body carry mechanical load over time.
A lateral positioning system adds controlled side to side movement for more complex positioning workflows.
These categories describe different operating principles. They do not represent a universal progression from basic to best.
Consider the Patient’s Ability to Move
A surface that allows greater immersion may improve pressure redistribution and comfort for some patients. The same characteristic may make independent movement or bed exit more difficult for others.
Patient strength, mobility and transfer method should therefore be considered alongside pressure redistribution performance.
The best surface is not necessarily the one that allows the greatest immersion. It is the one that provides appropriate support without creating an unnecessary barrier to movement and care.
Hospital Mattress Types Compared at a Glance
The following comparison presents the main mattress categories in a CMS friendly text format.
Pressure Redistribution Foam Mattress
Power requirement: Non powered
Primary function: Continuous reactive support and pressure redistribution
Typical advantages: Simple deployment, no pump, no alarm management and easier storage
Important checks: Foam density, firmness, envelopment, cover condition, bottoming out risk and bed compatibility
Relevant Optium example: FM 01 pressure redistribution foam mattress
Viscoelastic Mattress
Power requirement: Non powered
Primary function: Reactive support with greater body conformity and envelopment
Typical advantages: Comfort, pressure distribution and closer conformity to body contours
Important checks: Heat response, ease of movement, immersion, transfer requirements and cover performance
Relevant Optium example: FM 02 viscoelastic support surface
Low Air Loss Mattress
Power requirement: Powered
Primary function: Air based support with airflow that may assist pressure redistribution and microclimate management
Typical advantages: Variable air support and management of heat or moisture at the skin surface interface
Important checks: Pump controls, patient weight settings, airflow characteristics, noise, alarms, power interruption and maintenance
Relevant Optium example: FM 06 low air loss mattress system
Alternating Pressure Mattress
Power requirement: Powered
Primary function: Programmed inflation and deflation of air cells to change pressure loading over time
Typical advantages: Dynamic pressure redistribution, programmable cycles, monitoring and alarm functions
Important checks: Cycle settings, alarm response, CPR function, transport mode, cell replacement and staff training
Relevant Optium example: FM 08 alternating pressure therapy mattress
Lateral Air Mattress
Power requirement: Powered
Primary function: Dynamic pressure redistribution combined with assisted lateral positioning
Typical advantages: Alternating pressure, controlled right and left positioning and support for complex care workflows
Important checks: Positioning angle, patient tolerance, contraindications, alarm management, supervision and bed compatibility
Relevant Optium example: FM 10 lateral air mattress system
This comparison is an equipment overview, not a clinical prescription. Final selection should follow patient assessment, local policy and compatibility testing.
Foam Mattresses
A foam mattress is a non powered reactive support surface. Its material responds to the patient’s weight and body shape without using a pump.
Pressure redistribution foam should not be confused with basic foam that lacks appropriate support characteristics. Density alone also does not describe complete clinical performance.
Important variables include:
Foam composition
Layer construction
Cut pattern
Firmness
Envelopment
Recovery after compression
Cover elasticity
Patient weight range
The FM 01 Foam Mattress uses foam with a listed density of 32 kg/m³, CNC cut sections and internal air passages.
Optium lists a recommended thickness of 12 cm. The standard size is 195 × 85 × 12 cm, with a 200 × 85 × 12 cm option for Collesium Series hospital beds.
A non powered surface can reduce equipment complexity, but it still requires routine inspection. Foam fatigue, permanent indentation, fluid penetration and cover damage can reduce performance over time.
Viscoelastic Mattresses
A viscoelastic mattress is a reactive surface that responds to body weight and temperature. It is designed to conform more closely to the patient’s shape.
The FM 02 Viscoelastic Mattress combines an upper viscoelastic layer with a denser supporting layer. Its tube design includes air passages intended to support air circulation and reduce heat accumulation.
Optium lists an optimal thickness of 14 cm and a standard size of 195 × 85 cm.
Greater conformity can improve comfort for some users, but procurement teams should also consider whether the patient can reposition, transfer and leave the bed safely.
Surface performance should therefore be evaluated through both pressure management and patient movement.
Low Air Loss Mattresses
A low air loss mattress uses airflow through or around its air cells to support the patient and influence conditions at the skin surface interface.
The NPIAP, EPUAP and PPPIA guideline notes that the term “low air loss” describes a design feature, not a complete clinical performance claim.
The guideline encourages clinicians to compare standardised performance data related to pressure redistribution and microclimate management rather than relying only on the category label.
This is an important procurement distinction. Two mattresses marketed with the same term may not provide the same airflow, pressure behaviour, moisture management or alarm capabilities.
The FM 06 Low Air Loss Mattress contains 22 variable pressure cells, including six cells with an air ventilation system.
Its listed dimensions are 195 × 90 × 8 cm. The pump includes patient weight adjustment and is listed for patients weighing up to 180 kg.
Hospitals should still evaluate:
How pressure is controlled
Whether airflow is continuous or limited to selected cells
Which alarms are provided
How the system responds to a power failure
Whether the cover supports the intended airflow
How the system is cleaned and maintained
Alternating Pressure Mattresses
An alternating pressure mattress is a powered active support surface. Its air cells inflate and deflate in programmed cycles to change the distribution of pressure over time.
The clinical value of the system depends on more than the presence of moving air cells.
Staff must understand:
Patient weight or comfort settings
Cycle duration
Low pressure alarms
Power failure alarms
CPR operation
Transport mode
Care or firm mode
The response required when a cell fails
The FM 08 Therapy Mattress uses 18 replaceable polyurethane air cells.
Its system provides selectable pressure cycles of 10, 15, 20 and 25 minutes. Listed functions include audible and visual alarms, position sensing, automatic weight detection, a CPR valve, transport mode and a removable four way stretch cover.
The product page does not currently state the total mattress thickness. This measurement should therefore be confirmed with Optium before compatibility or side rail assessments are completed.
Lateral Air Mattresses
A lateral air mattress combines dynamic pressure redistribution with controlled right and left positioning.
The FM 10 Lateral Air Mattress uses 18 variable pressure cells and provides selectable pressure cycles of 10, 15, 20 and 25 minutes.
Its secondary positioning system can move the patient up to 30 degrees to the right or left. Listed features include position sensing, weight detection, transport mode, alarms, rapid air release and replaceable cells.
Lateral positioning technology may support demanding care workflows, but it should not be treated as an automatic replacement for manual assessment or caregiver supervision.
Hospitals should evaluate patient tolerance, bed compatibility, safe positioning protocols and clinical contraindications before deployment.
The product page does not currently list the complete mattress thickness. This should be confirmed during technical evaluation.
Editorial Transparency About Product Examples
The clinical principles in this guide are based on independent sources including the NPIAP, EPUAP and PPPIA International Pressure Injury Guideline, NICE, AHRQ and FDA guidance.
Optium products are included as examples of equipment within each support surface category. Product descriptions do not replace independent clinical assessment, local hospital policy or professional judgement.
Manufacturer statements concerning risk categories or pressure injury prevention should always be interpreted within this wider clinical context.
No Hospital Mattress Replaces Repositioning
No support surface completely removes the need for repositioning.
The NPIAP, EPUAP and PPPIA repositioning guideline states that individuals at risk should continue to be repositioned regardless of the type of pressure redistribution surface in use.
The guideline explains that repositioning intervals may be adjusted according to:
Patient mobility
Ability to reposition independently
Skin and tissue tolerance
Clinical condition
Comfort
Sleep patterns
Goals of care
The support surface being used
It conditionally suggests that intervals of either two or three hours may be appropriate for many at risk individuals who are already using a suitable pressure redistribution surface.
However, this recommendation is based on very low certainty evidence and must be individualised. It should not be converted into a universal turning schedule.
A complete prevention strategy may include:
Individual risk assessment
Regular skin and tissue inspection
Clinically appropriate repositioning
Heel protection where required
Moisture and continence management
Nutrition and hydration support
Safe mobilisation
Clear documentation and handover
Hospitals can connect mattress planning with Optium’s guide to patient falls and hospital bed safety, where mattress fit, bed height and room layout are considered as parts of the same safety system.
Why Mattress and Hospital Bed Compatibility Is a Safety Issue
A medical mattress for a hospital bed must fit the actual bed frame. Matching only an approximate width and length is not sufficient.
An incompatible mattress can affect:
Gaps between the mattress and side rails
Effective patient surface height
Side rail protection
Bed articulation
Transfer height
Mattress movement on the platform
Access to CPR or emergency functions
The position of securing straps and cables
The FDA hospital bed system guidance warns that replacing an original mattress or side rail may change gaps within the complete bed system and increase entrapment risk.
For this reason, the bed, mattress and side rails should be assessed as one system.
Before approval, facilities should test the mattress with the bed in:
Flat position
Backrest elevated position
Knee break position
Lowest height
Highest height
Transfer position
Emergency CPR position
Transport configuration
Powered surfaces should also be assessed during power interruption and while the bed is operating on battery power.
Further positioning and workflow considerations are discussed in Optium’s guide to electric hospital beds for postoperative recovery.
The Optium Five Fit Mattress Test
For this guide, Optium frames mattress selection through five forms of fit.
1. Patient Fit
Does the surface suit the patient’s mobility, pressure injury risk, body dimensions, comfort requirements and ability to reposition?
2. Pressure Fit
Does the surface provide the required form of pressure redistribution, envelopment, immersion, airflow, alternating pressure or lateral movement?
3. Platform Fit
Are the mattress dimensions, thickness, securing method and articulation compatible with the bed frame and side rails?
4. Protocol Fit
Can nursing, infection prevention, biomedical and environmental services teams use, clean, inspect and maintain the system within existing procedures?
5. Procurement Fit
Are covers, pumps, cells, spare parts, technical support and training available throughout the expected service life?
A mattress passes the test only when it fits all five areas.
Strong technology can still become a poor investment when it does not fit the patient, bed, workflow or maintenance system.
Optium Hospital Mattress Product Comparison
The following text comparison summarises five Optium support surface options without using a table.
FM 01 Foam Mattress
Operating type: Non powered reactive foam
Listed thickness: 12 cm
Listed standard dimensions: 195 × 85 × 12 cm
Primary evaluation context: General non powered support, pressure redistribution, simple deployment and compatibility with hospital bed articulation
Key features: 32 kg/m³ foam, CNC cut sections, internal air passages, reversible construction and breathable waterproof cover
FM 02 Viscoelastic Mattress
Operating type: Non powered reactive viscoelastic foam
Listed thickness: 14 cm
Listed standard dimensions: 195 × 85 cm
Primary evaluation context: Greater envelopment, patient comfort and reactive pressure distribution
Key features: Viscoelastic upper layer, denser supporting layer, tube design, internal air passages and antistatic cover
Explore the FM 02 viscoelastic mattress
FM 06 Low Air Loss Mattress
Operating type: Powered variable pressure air system
Listed thickness: 8 cm
Listed dimensions: 195 × 90 × 8 cm
Primary evaluation context: Variable air support and evaluation of microclimate related requirements
Key features: 22 air cells, six ventilated cells, patient weight adjustment and listed capacity up to 180 kg
Review the FM 06 low air loss system
FM 08 Therapy Mattress
Operating type: Powered alternating pressure system
Listed thickness: Not stated on the current product page
Primary evaluation context: Programmable dynamic pressure redistribution and monitored powered therapy
Key features: 18 replaceable cells, four selectable cycle durations, alarms, position sensing, automatic weight detection, CPR valve and transport mode
See the FM 08 alternating pressure mattress
FM 10 Lateral Air Mattress
Operating type: Powered alternating pressure and lateral positioning system
Listed thickness: Not stated on the current product page
Primary evaluation context: Dynamic pressure redistribution combined with assisted right and left positioning
Key features: 18 variable pressure cells, four selectable cycle durations, movement up to 30 degrees, alarms, weight detection, transport mode and replaceable cells
Examine the FM 10 lateral air system
These product examples provide starting points for technical evaluation. Final suitability must be confirmed against the intended patient group, hospital bed and clinical protocol.
What Procurement Teams Should Compare Beyond Purchase Price
Cover Construction
Review fluid resistance, breathability, elasticity, seams, zipper design and compatibility with approved cleaning agents.
A cover is part of the clinical support surface. It should not be treated as packaging.
Internal Inspection
Determine how staff will identify foam breakdown, damaged cells, contamination, loss of pressure or fluid penetration.
The inspection process should include clear criteria for removing a mattress from service.
Pump and Alarm Functions
For powered systems, review:
Low pressure alarms
Power fault warnings
Automatic control locking
Weight or comfort settings
Position sensing
Display clarity
Alarm volume
Ease of troubleshooting
Cleaning and Care Modes
Check whether the system provides a firm mode for care, cleaning or transfers.
Confirm whether covers can be removed and replaced without unnecessary equipment downtime.
Replaceable Components
Replaceable cells, covers and pumps can reduce downtime and lifecycle cost.
The hospital should confirm which components can be changed on site and which repairs require authorised service.
Transport and Power Failure
Clarify how long pressure is retained during transport and what happens when power is interrupted.
Transport mode should be tested under the facility’s actual transfer conditions.
Training Requirements
A complex mattress creates value only when nurses, porters, biomedical teams and cleaning personnel understand how to use it.
Training should include routine use, alarms, CPR release, transport, cleaning, fault reporting and mattress inspection.
Total Cost of Ownership
The complete cost may include:
Replacement covers
Replacement cells
Pumps
Preventive maintenance
Staff training
Storage
Cleaning
Technical service
Downtime
Replacement frequency
The same lifecycle principle is explored in Optium’s hospital bed price and long term ownership comparison.
Common Hospital Mattress Procurement Mistakes
Selecting One Mattress for Every Department
A general ward, emergency department, intensive care unit and long term care environment may have different patient profiles and support requirements.
Standardisation can simplify procurement, but excessive standardisation may produce a poor clinical fit.
Buying Technology Without a Clinical Protocol
An alternating pressure mattress cannot produce consistent value when settings, alarms, repositioning responsibilities and escalation procedures are unclear.
Technology and protocol must be purchased together.
Ignoring Mattress Thickness
Mattress thickness changes the effective patient height.
It can influence side rail protection, transfers, overbed table positioning and the patient’s ability to enter or leave the bed.
Assuming Low Air Loss and Alternating Pressure Are the Same
Airflow and pressure cycling are different functions.
Some systems combine both. Others provide only one. Product category names should therefore be checked against actual performance and design characteristics.
Treating the Mattress Cover as Packaging
The cover influences friction, shear, cleaning, moisture protection and mattress durability.
Damage, stretching, fluid penetration or incompatible disinfectants can affect both hygiene and performance.
Comparing Only Initial Price
A lower purchase price may create higher long term costs if covers fail early, cells cannot be replaced, pumps cannot be repaired or spare parts are unavailable.
Hospital Mattress Procurement Checklist
Before placing an order, confirm:
Which departments will use the mattress?
What patient risk profiles are expected?
Is the surface reactive, active or a combination?
What pressure redistribution properties are required?
Does the mattress fit the bed dimensions exactly?
Does its thickness preserve safe side rail geometry?
Can it follow every intended bed movement?
How is it secured to the platform?
Is the cover removable?
Is the cover compatible with hospital disinfectants?
How will internal damage be detected?
Are cells, covers and pumps replaceable?
What alarms and emergency functions are included?
What happens during transport?
What happens during a power failure?
Who will train clinical, cleaning and technical teams?
What preventive maintenance is required?
How will damaged mattresses be removed from service?
What spare part support is available?
What is the expected total ownership cost?
Conclusion
A hospital bed supports positioning and movement. The mattress determines how the patient experiences that support during every hour spent in bed.
The right choice begins with patient risk, not with product category or price. It continues through pressure redistribution, bed compatibility, repositioning protocol, hygiene, maintenance and staff training.
Optium offers foam, viscoelastic and powered hospital mattress systems for different care environments and support requirements.
Hospital procurement teams, nursing leaders and project planners can review the Optium medical equipment catalogue or contact Optium to compare mattress configurations with the intended bed, patient group and care workflow.
Frequently Asked Questions
What Is the Best Type of Hospital Mattress?
There is no single best mattress for every patient.
The correct surface depends on pressure injury risk, mobility, skin condition, moisture, body dimensions, comfort and the patient’s ability to reposition.
What Is the Difference Between a Foam and Alternating Pressure Mattress?
A foam mattress redistributes pressure through its material and structure.
An alternating pressure mattress uses powered air cells that inflate and deflate in programmed cycles.
When Should a Low Air Loss Mattress Be Considered?
A low air loss mattress may be considered when pressure redistribution and skin surface microclimate are important.
Selection should follow clinical assessment and comparison of actual performance characteristics rather than the product label alone.
Can an Alternating Pressure Mattress Prevent Pressure Injuries?
No mattress can guarantee pressure injury prevention.
An alternating pressure system can support a wider prevention plan that also includes assessment, repositioning, skin care, nutrition and monitoring.
Does Every Hospital Mattress Fit Every Hospital Bed?
No.
Length, width, thickness, side rail geometry, securing method and articulation must all be checked before the mattress is approved.
Does a Dynamic Mattress Eliminate the Need to Turn a Patient?
No.
Current NPIAP, EPUAP and PPPIA guidance states that no support surface can entirely replace individualised repositioning.
How Often Should a Patient Be Repositioned?
There is no universal schedule for every patient.
Current guidance states that timing should be individualised according to mobility, skin tolerance, clinical condition, comfort and the support surface in use.
How Often Should a Hospital Mattress Be Replaced?
There is no universal replacement interval.
A mattress should be removed when inspection identifies contamination, permanent deformation, cover failure, damaged cells, loss of pressure or performance that no longer meets clinical requirements.
What Should Buyers Check in a Powered Mattress Pump?
Buyers should check alarms, pressure settings, weight adjustment, CPR release, transport mode, control locking, position sensing, maintenance requirements and spare part availability.
Is a More Expensive Hospital Mattress Always Better?
No.
The more appropriate mattress is the one that fits the patient, bed, clinical protocol and service infrastructure without unnecessary complexity.
Sources and Methodology
This article separates independent clinical guidance from manufacturer product information.
It does not claim that any mattress independently prevents pressure injuries, treats a medical condition or replaces patient assessment and repositioning.
Key clinical sources:
NPIAP, EPUAP and PPPIA International Pressure Injury Guideline: Full Body Support Surfaces
NPIAP, EPUAP and PPPIA International Pressure Injury Guideline: Repositioning
NICE: Pressure Ulcers, Prevention and Management
AHRQ: Pressure Injury Prevention Program Implementation Guide
FDA: Hospital Bed System Dimensional and Assessment Guidance