
Choosing an electric hospital bed is not only a product comparison. For hospital procurement teams, biomedical engineers, ICU managers and ward managers, the right bed affects patient safety, caregiver workflow, cleaning routines, positioning flexibility, maintenance planning and long-term operational value.
A low-acuity ward does not need the same electric bed as an ICU-adjacent recovery area. A post-op unit does not evaluate beds in the same way as a high-dependency care environment. That is why a strong hospital bed buying checklist should start with clinical use, not with model names.
This guide gives hospital buyers 53 practical questions to ask before choosing an electric hospital bed. Use it to compare technical specifications, department needs and supplier support before making a procurement decision.
For buyers comparing the Optium Collesium Series, these questions can also help match the right model to the right care environment.
Quick navigation
Use this guide by section:
Clinical use and department fit
Patient safety and fall prevention
Positioning and electric functions
Caregiver ergonomics and ward workflow
Side rails, patient access and control panels
Mobility, castors and braking
Hygiene, cleaning and room turnover
Mattress and pressure care compatibility
Electrical system, battery and durability
Standards, documentation and biomedical approval
Maintenance, spare parts and total cost of ownership
Optium Collesium model guidance
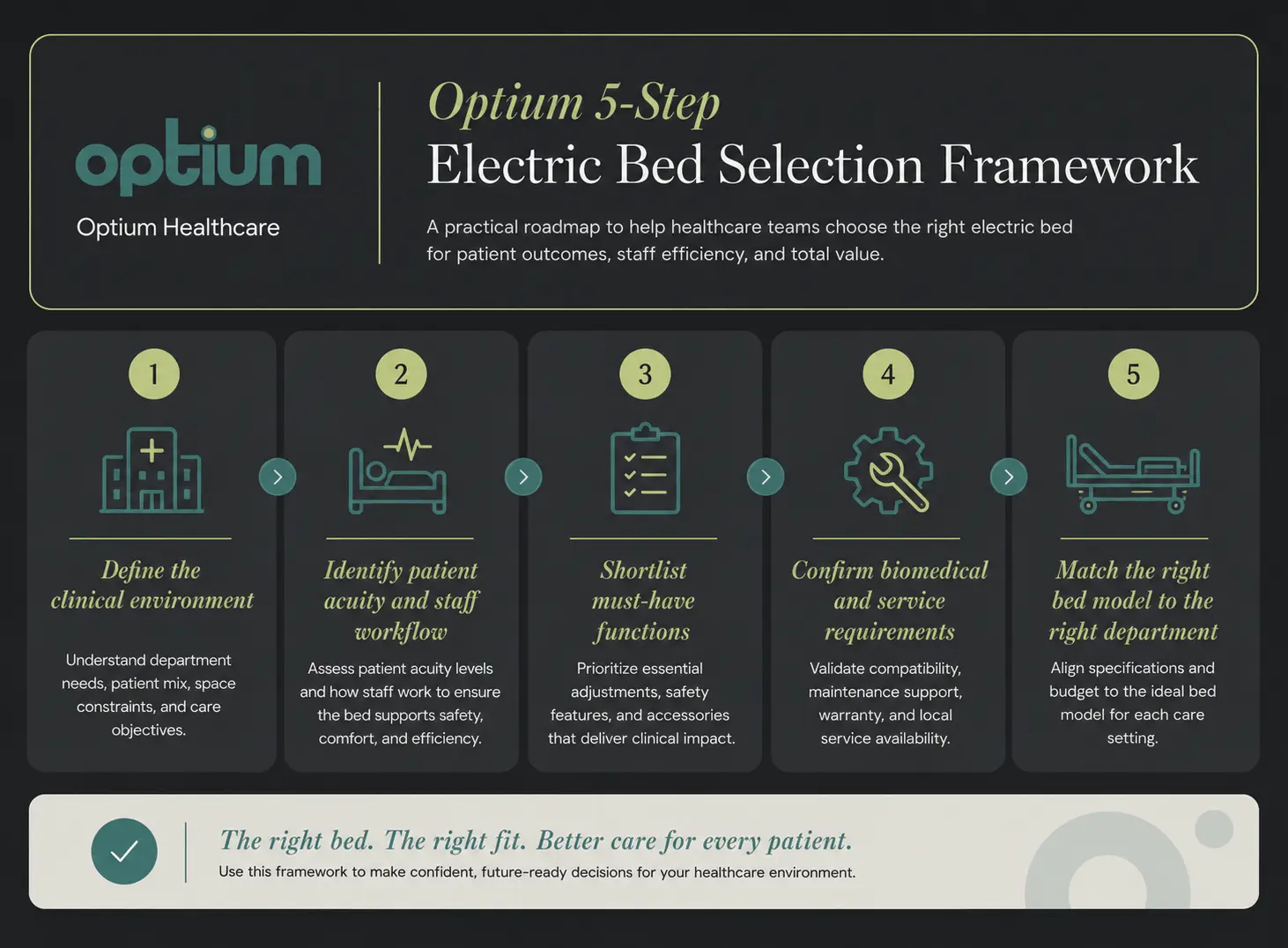
The Optium 5-Step Electric Bed Selection Framework
A structured electric bed selection process helps hospitals avoid two common mistakes: under-specifying beds for high-acuity areas and over-specifying beds for standard wards.
Under-specifying creates workflow friction. Staff may lack the positioning, braking, cleaning or control features they need every day. Over-specifying creates unnecessary cost and complexity when a simpler electric patient care bed would support the department properly.
Optium’s 5-step framework is simple:
Define the clinical environment first
Identify patient acuity and staff workflow
Shortlist must-have functions
Confirm biomedical and service requirements
Match the right bed model to the right department
This framework keeps the procurement process practical. Instead of asking “Which bed has the most functions?”, buyers can ask “Which bed fits this department’s real care workflow?”
Questions for clinical use and department fit
Start by asking where the bed will be used. This is the most important decision layer because every other feature depends on the department’s workflow.
1. Which department will use the bed most often?
The department determines the bed specification. A standard ward, ICU, surgical recovery unit, step-down room and long-stay patient area each need a different feature level.
For example:
Standard wards usually need reliable electric positioning and hygiene-friendly design
Post-op recovery units need height adjustment, side rails and smooth repositioning
Step-down rooms need more advanced control and positioning functions
ICU-adjacent rooms need nurse control, emergency positioning and stronger mobility features
2. What is the typical patient acuity level?
Patient acuity should guide the bed choice. Low-acuity patients usually need basic electric positioning, while high-acuity patients often require nurse control, Trendelenburg, reverse Trendelenburg, CPR functions, lateral tilt or battery backup.
A simple way to classify need:
Low acuity: basic patient care and comfort positioning
Moderate acuity: post-op, recovery or step-down support
High acuity: ICU-adjacent or high-dependency care
3. Will the bed be used for post-surgery recovery?
For post-surgery recovery, prioritize transfer safety, height adjustment, backrest and legrest positioning, side rail safety, cleaning access and caregiver ergonomics.
Post-surgery patients can be weak, dizzy, in pain or limited in movement. The bed should help nurses reposition and observe patients without adding unnecessary physical strain. For a deeper post-op buying guide, see Optium’s article on electric hospital beds for post-surgery recovery.
4. Will the bed be used in ICU or ICU-adjacent care?
For ICU or ICU-adjacent care, buyers should look beyond basic motor count. The priority is faster clinical control, safer positioning and better access for staff.
Key features to evaluate include:
Nurse control
One-touch positioning
Central locking
Lateral tilt
X-ray cassette holder
Battery backup
Emergency positioning functions
Embedded side rail controls
These functions matter most when staff need closer observation and more complex positioning.
5. Does the hospital need one bed type or a mixed model strategy?
Most hospitals benefit from a mixed model strategy. One bed type rarely fits every department well.
A stronger approach is to match model level to department need:
Simpler electric patient care beds for lower-acuity rooms
3-motor electric beds for standard wards and post-op units
4-motor electric beds for step-down and higher-acuity care
5-motor ICU beds for high-dependency and ICU-adjacent environments
Questions for patient safety and fall prevention
An electric bed does not prevent falls on its own. Fall prevention is a wider care process involving bed height, brakes, lighting, footwear, observation, room layout and staff workflow.
The AHRQ falls topic page states that between 700,000 and 1,000,000 people fall in U.S. hospitals each year. The AHRQ Patient Safety Network also notes that more than one-third of in-hospital falls result in injury, including serious injuries such as fractures and head trauma.
For procurement teams, this does not mean “the bed solves fall risk.” It means bed height, brakes, side rails, controls and transfer workflow should be reviewed as part of the hospital’s wider fall-prevention process.
6. Can the bed lower enough for safer patient access?
The bed should lower enough to support safer entry and exit. This is especially important for weak, elderly, post-op or mobility-limited patients.
A low resting height can support patient access, while a higher working height supports caregiver tasks.
7. Can the bed rise high enough for caregiver tasks?
The bed should rise to a comfortable working height for nurses and caregivers. This matters during wound checks, repositioning, hygiene routines and transfer preparation.
A bed that stays too low forces staff into awkward positions. Over time, that affects caregiver ergonomics and workflow efficiency.
8. Are the brakes easy to activate and verify?
Brakes should be easy to activate, easy to see and easy to trust. A braking system that is hard to use will not support daily safety routines.
Buyers should check:
Brake pedal position
Locking feedback
Staff access from normal working positions
Whether central locking is available
Whether the brake system feels stable during transfer
9. Does the bed have central locking or diagonal locking?
The bed should have the right locking system for its department. Central locking is stronger for higher-acuity or frequently moved environments. Diagonal locking can be enough for lower-acuity rooms with simpler workflows.
For ICU, step-down and high-dependency care, central locking is usually the better procurement target.
10. Are protective bumpers included?
Protective bumpers are useful in hospital environments where beds move through rooms, doorways, corridors and cleaning areas.
They help reduce impact during movement and protect both the bed and surrounding surfaces.
11. Does the bed support safer bed-exit workflows?
For high-acuity environments, buyers should check whether the bed includes bed-exit positioning or related staff control functions.
Bed-exit support is not needed in every ward, but it becomes more relevant when patients need closer observation, assisted mobilization or faster staff control.
Questions for positioning and electric functions
Positioning is one of the main reasons hospitals buy electric beds. Buyers should focus on the positions the department actually uses, not only the number of motors.
Trendelenburg means the bed tilts so the head side is lower than the foot side. Reverse Trendelenburg means the head side is higher than the foot side. Fowler position means the backrest is raised to support a semi-sitting posture. Vascular position usually refers to leg elevation for lower-limb support when clinically appropriate.
12. Which sections are electrically adjustable?
Buyers should confirm which bed sections move electrically before comparing models. The most common adjustable areas are:
Backrest
Height
Legrest
Trendelenburg / reverse Trendelenburg
Lateral tilt on advanced ICU beds
A bed with more electric sections gives staff more control, but only if those functions match the department’s real workflow.
13. Is electric height adjustment included?
Electric height adjustment should be included for most standard ward, post-op and high-acuity care environments.
Some lower-acuity models may include electric backrest and legrest adjustment without full electric height adjustment. That can be acceptable in simpler rooms, but it is not ideal for high-transfer or high-care workflows.
14. Does the bed support Fowler position?
Fowler positioning is important for many daily care routines. It supports sitting posture for meals, communication, breathing comfort and observation.
For standard wards and post-op recovery, Fowler position is usually a core requirement.
15. Does the bed support vascular position?
Vascular position matters when the unit frequently needs lower-limb support. It can help support leg elevation when clinically appropriate.
Buyers should confirm whether the position is supported by the bed’s electric functions or by manual adjustment.
16. Are Trendelenburg and reverse Trendelenburg required?
Trendelenburg and reverse Trendelenburg are mainly required in higher-acuity areas such as ICU, step-down and high-dependency care.
Before specifying these functions, ask:
Does the department protocol require them?
Will staff use them regularly?
Are angle indicators available?
Is nurse control needed for these positions?
17. Does the bed include auto-contour?
Auto-contour is useful because it coordinates bed sections to create a more supported sitting position.
In practical terms, auto-contour helps the bed move more naturally when the patient is raised into a seated posture. It can reduce manual adjustment and improve positioning consistency.
18. Does the bed include auto-regression?
Auto-regression is useful because it allows the backrest area to move in a way that helps reduce sliding and compression when the backrest is raised.
For post-op and high-acuity patients, this can make repositioning smoother and reduce unnecessary handling.
Questions for caregiver ergonomics and ward workflow
A bed should support the people using it every day. Nurse workflow, control access and repeated bedside tasks are major procurement considerations.
19. Can staff adjust the bed quickly during routine care?
Common functions should be accessible quickly. If backrest, height or legrest adjustment takes too many steps, routine care slows down.
Buyers should test the real workflow:
Raise the backrest
Lower the bed for patient access
Raise the bed for nursing care
Move into Fowler position
Return to flat position
Lock and unlock the brakes
If these steps feel slow during a demonstration, they will feel slower in daily ward use.
20. Is a nurse control unit included or optional?
Nurse control is important in higher-acuity areas. It gives staff faster and more centralized control over bed functions.
For standard wards, a patient handset may be enough. For step-down, ICU-adjacent or high-dependency care, nurse control should be strongly considered.
21. Are one-touch functions available?
One-touch functions are valuable when the department needs faster positioning and more consistent staff response.
Useful one-touch functions can include:
CPR
Examination position
Cardiac chair
Bed-exit position
Shock position
Semi-Fowler position
These functions are not necessary for every room, but they matter in high-acuity care where staff need speed and consistency.
22. Is manual CPR available?
Manual CPR is important for emergency response. Dual-sided manual CPR levers can help staff flatten the backrest quickly when needed.
For high-acuity units, buyers should check both electronic CPR and manual CPR availability.
23. Are controls intuitive for both staff and patients?
Controls should be easy to understand. Complex controls increase training needs and can slow down routine care.
The best control interface is clear, accessible and protected against accidental use.
24. Is there an activation key or lockout function?
Advanced beds should include activation or lockout functions. These help prevent undesired positioning, especially when multiple electric functions and side rail controls are available.
Questions for side rails, patient access and control panels
Side rails are not just safety accessories. Their design affects cleaning, transfers, nurse access and patient confidence.
25. Are the side rails lockable?
Side rails should be lockable. A secure locking system helps ensure the rail remains stable when raised.
Buyers should test the side rail mechanism during product evaluation, not only read the specification.
26. Are side rails easy to lower, fold away or tuck away?
Side rails should lower or tuck away smoothly. Staff still need access for wound checks, linen changes, hygiene care and transfers.
A side rail that protects the patient but blocks care access creates workflow friction.
27. Are side rails easy to clean?
Side rails should be easy to clean and inspect. Smooth PP side rail designs can support hygiene routines between patients.
Buyers should check for:
Smooth surfaces
Minimal hard-to-clean gaps
Accessible hinge areas
Compatible cleaning guidance
Removable or serviceable components
28. Do side rails include embedded controls?
Embedded side rail controls are useful in higher-acuity models. They give patients and nursing staff easier access to key bed functions.
This feature is especially relevant for ICU and high-dependency care environments.
29. Do side rails block transfer or bedside care?
Side rails should not block safe transfer or routine bedside care. The best side rail system supports protection without making staff access difficult.
During evaluation, procurement teams should ask nurses to simulate real care tasks around the bed.
Questions for mobility, castors and braking
Even when beds stay in one unit, castors and brakes still matter. Beds move during cleaning, transfers, repositioning, room changes and service access.
30. What castor size does the bed use?
Castor size matters because it affects movement and handling. Larger castors can support smoother movement, especially in higher-acuity or frequently moved environments.
For example, several higher-acuity Optium Collesium models list central lockable 150 mm castors.
31. Are the castors diagonal lockable or central lockable?
The locking system should match the department’s risk and movement profile.
Use this logic:
Diagonal locking: suitable for simpler, lower-acuity rooms
Central locking: stronger for ICUs, step-down rooms and frequently moved beds
Central locking with larger castors: better for high-dependency environments
32. Is the brake system easy to access from normal working positions?
Staff should be able to lock and unlock the bed without awkward movement.
A brake system that requires bending, searching or repositioning is less likely to be used consistently.
33. Does the bed stay stable when locked?
The bed should feel stable when locked. Stability affects transfers, repositioning and bedside procedures.
During evaluation, test the bed in raised, lowered and flat positions.
34. Are castors serviceable and replaceable?
Castors should be serviceable and replaceable. They experience daily wear, especially in hospitals where beds move often.
Biomedical teams should confirm replacement availability before purchase.
Questions for hygiene, cleaning and room turnover
Cleaning is part of bed performance. The CDC environmental cleaning guidance covers cleaning procedures in patient care areas and for noncritical patient care equipment, which makes cleanable bed design a practical buying requirement.
35. Are the headboard and footboard removable?
Removable headboards and footboards make access, cleaning and maintenance easier.
They also support faster response in certain care situations where staff need better access to the patient.
36. Is the mattress platform removable?
A removable mattress platform can improve cleaning access and room turnover routines.
Buyers should check whether the platform sections are easy to remove, clean and reinstall.
37. Are there unnecessary crevices or hard-to-clean areas?
The bed should avoid unnecessary crevices, gaps and hard-to-clean surfaces.
Complex shapes can slow cleaning and create maintenance issues over time.
38. Are side rails, panels and surfaces compatible with hospital cleaning routines?
Bed materials should be compatible with the hospital’s cleaning and disinfection protocols.
Procurement teams should request cleaning guidance before purchase, especially for side rails, ABS platforms, PP panels and painted metal frames.
39. Is the frame finish suitable for repeated hospital use?
The frame finish should be suitable for repeated cleaning and long-term hospital use.
Electrostatic powder-coated or epoxy-painted metal frames are common in hospital bed designs, but buyers should confirm durability, maintenance and cleaning guidance.
Questions for mattress and pressure care compatibility
The bed and mattress should be evaluated together. The bed frame does not replace clinical pressure injury prevention, but it affects how well support surfaces fit and function.
The NICE pressure ulcer prevention guidance highlights the importance of appropriate support surfaces for at-risk patients and surgical patients.
40. What mattress size is compatible with the bed?
Mattress size must match the bed. A poor mattress fit can affect patient comfort, side rail performance and safety.
Buyers should confirm mattress dimensions, platform compatibility and recommended mattress types.
41. Does the platform support the hospital’s required mattress type?
The platform should support the mattress type approved by the hospital.
This can include:
Standard foam mattresses
High-specification foam mattresses
Pressure-redistributing surfaces
Department-specific support surfaces
42. Does the bed design support stable patient positioning?
The bed should support stable positioning through its backrest, legrest, height adjustment, auto-contour and platform design.
A stable platform makes daily repositioning easier for staff and more comfortable for patients.
43. Is bed extension required?
Bed extension is useful when the hospital serves taller patients or varied patient profiles.
If bed extension is optional, buyers should decide whether it is needed during the tender stage, not after purchase.
Questions for electrical system, battery and durability
Electrical performance matters because hospital beds are used repeatedly over many years.
44. What IP protection standard is listed for the electronic system?
The IP protection standard helps buyers understand the electronic system’s resistance to environmental exposure.
Several Optium Collesium models list IPX6 standard electronic systems. Biomedical teams should confirm what this means for the hospital’s cleaning and use environment.
45. Is battery backup included or optional?
Battery backup should be included or available when beds need to move, when power continuity is a concern or when emergency functions must remain available.
For high-acuity rooms, battery backup should be treated as a major decision point.
46. Are motors and actuators serviceable?
Motors and actuators should be serviceable. Biomedical teams should confirm replacement process, spare parts availability and technical documentation.
A feature-rich bed loses value if key components are difficult to maintain.
47. Is there protection against undesired positioning?
Advanced beds should include protection against undesired positioning.
Look for:
Activation key
Lockout function
Nurse control priority
Protected side rail controls
Clear control labeling
48. Does the bed include angle indicators?
Angle indicators are useful in higher-acuity environments. They help staff monitor backrest, Trendelenburg and reverse Trendelenburg positions more clearly.
For ICU-adjacent care, angle indicators should be part of the comparison.
Questions for standards, documentation and biomedical approval
Procurement should not stop at feature comparison. Biomedical approval and documentation review are essential before purchase.
49. Is technical documentation available?
Technical documentation should be available before purchase.
Request:
Product specifications
User manual
Cleaning guidance
Service information
Spare part details
Electrical system information
Optional configuration list
50. Are CE, quality and regulatory documents available where required?
Hospitals should confirm documentation according to their country, tender and import requirements.
Do not rely only on marketing claims. Ask for the documents required by the procurement process.
51. Has the biomedical engineering team reviewed the bed?
The biomedical engineering team should review the bed before approval.
The review should cover:
Electrical system
Controls
Castors
Brakes
Side rails
Serviceability
Spare parts
Cleaning compatibility
Mattress compatibility
Department fit
Maintenance, spare parts and total cost of ownership: questions 52–53
The cheapest bed at purchase is not always the lowest-cost bed over time. Total cost of ownership includes serviceability, downtime, cleaning time, spare parts and training.
52. Are spare parts available for the expected lifecycle?
Spare parts should be available for the expected lifecycle of the bed.
Check availability for:
Side rails
Castors
Control units
Actuators
IV poles
Bumpers
Headboards and footboards
Platform sections
Battery components
53. Does the supplier provide project and configuration support?
The supplier should help match models to departments, not simply sell one bed type for every room.
For hospital projects, configuration support can help procurement teams avoid both over-specification and under-specification.
How to use these 53 questions in a real procurement process
Use this checklist in three steps.
First, define the department. Separate standard wards, post-op recovery units, ICU-adjacent rooms and high-dependency care areas.
Second, shortlist functions. Decide which rooms need height adjustment, Trendelenburg, nurse control, one-touch positions, lateral tilt, battery backup, X-ray cassette holder or central locking.
Third, match models to acuity. In the Optium Collesium range, lower-acuity rooms can be reviewed with models such as CL 22, standard post-op and patient care rooms with CL 32, step-down and higher-acuity rooms with CL 41 or CL 42, and ICU-adjacent environments with CL 45, CL 50 or CL 55.
For a more function-focused comparison, you can also read Optium’s guide to 3-motor vs 4-motor hospital beds.
Quick Collesium model comparison
Use this model guide as a procurement shortlist, not as a final technical approval document. Biomedical teams should confirm the final configuration and product sheet before purchase.
CL 22: lower-acuity patient care
Model: CL 22 Electronic Patient Care Bed, 2 Motors
Motor level: 2 motors
Target environment: lower-acuity patient care
Main distinction: electric backrest and legrest support for simpler care workflows
Best fit: rooms where full electric height adjustment is not required
CL 32: standard electric patient care
Model: CL 32 Electronic Patient Care Bed, 3 Motors
Motor level: 3 motors
Target environment: standard patient care and post-op wards
Main distinction: electric height adjustment, Fowler and vascular positions, auto-contour and auto-regression
Best fit: standard wards that need reliable daily positioning and caregiver access
CL 41: step-down and higher-acuity care
Model: CL 41 Electronic ICU and Patient Care Bed, 4 Motors
Motor level: 4 motors
Target environment: step-down and higher-acuity care
Main distinction: Trendelenburg and reverse Trendelenburg with optional nurse control and optional X-ray cassette holder
Best fit: units that need more positioning capability than a standard 3-motor bed
CL 42: higher-acuity care with foot-end nurse control
Model: CL 42 Electronic ICU Bed, 4 Motors
Motor level: 4 motors
Target environment: higher-acuity care and step-down rooms
Main distinction: foot-end nurse control, one-button examination position and electronic CPR
Best fit: departments where staff need faster control from the foot end of the bed
CL 45: advanced recovery and ICU-adjacent care
Model: CL 45 Electronic ICU Bed, Column Motors
Motor level: column motor system
Target environment: advanced recovery and ICU-adjacent care
Main distinction: embedded side rail controls, X-ray translucent HPL backrest, battery backup and optional integrated weight scale
Best fit: high-dependency units that need advanced positioning and stronger staff control
CL 50 / CL 55: high-acuity ICU-level care
Models: CL 50 Electronic ICU Bed, 5 Motors and CL 55 Electronic ICU Bed, 5 Motors
Motor level: 5 motors
Target environment: high-acuity ICU-level care
Main distinction: lateral tilt, one-touch positioning, X-ray cassette holder, rechargeable battery backup and 150 mm central lockable castors
Best fit: ICU-adjacent or high-dependency care environments that need advanced positioning and staff control
Procurement note: CL 50 and CL 55 should be compared with Optium’s model-specific technical documentation before final approval. Public product information lists a similar core feature set, so the final choice should be based on project configuration, technical requirements and Optium’s product recommendation.
FAQ
What is the most important question before buying an electric hospital bed?
The most important question is where the bed will be used. Department fit determines whether the hospital needs a basic electric patient care bed, a post-op recovery bed, a step-down bed or an ICU-level electric hospital bed.
How many motors should an electric hospital bed have?
The right motor count depends on the clinical workflow. A 3-motor bed can support many standard ward and post-op needs. A 4-motor or 5-motor bed is more relevant when the department needs Trendelenburg, reverse Trendelenburg, nurse control, lateral tilt or advanced one-touch functions.
What should procurement teams check besides price?
Procurement teams should check department fit, positioning functions, side rails, brakes, castors, cleaning access, mattress compatibility, battery backup, serviceability, spare parts and supplier support.
Why is height adjustment important in hospital beds?
Height adjustment supports safer patient access and better caregiver ergonomics. It allows the bed to lower for patient entry and exit, then rise for bedside care tasks.
Should every hospital room use the same electric bed?
Not always. A mixed model strategy is often better. Standard wards, post-op units, step-down rooms and ICU-adjacent areas usually need different feature levels.
Which Optium electric hospital bed should buyers compare first?
Start with the department. CL 32 is a practical starting point for standard electric patient care. CL 41 and CL 42 suit higher-acuity and step-down care. CL 45, CL 50 and CL 55 are stronger fits for ICU-adjacent or high-acuity environments.
Final CTA
Need help choosing the right electric hospital bed configuration for your project?
Contact Optium to compare Collesium models by department, patient acuity, positioning needs, hygiene workflow, mobility requirements and long-term service expectations.